Osseonews: Dr. Balshi, from your description of your technique it appears that it is critical for you to determine if the implant fixture has achieved adequate primary stability before you deliver the prosthesis.
Dr. Balshi: Achieving primary stability is critical. We need to know that the implant fixture is securely locked into the surrounding bone in the initial stage. Secondary stability will be achieved later over time. If we determine that an implant fixture has not achieved primary stability, we have to treat it differently.
Osseonews: Could you describe your protocol for determining primary stability?
Dr. Balshi: In the majority of current treatment applications insertion torque generally provides the stability quantification. However in research cases we use Resonance Frequency Analysis (RFA). This provides an accurate, quantitative assessment of the quality of the implant fixture to bone interface. In essence we transmit mechanical vibrations to the implant to bone interface. We then monitor changes in resonance frequency. This provides a very accurate assessment of the stability of the implant in the bone.
Osseonews: How do you deploy this system?
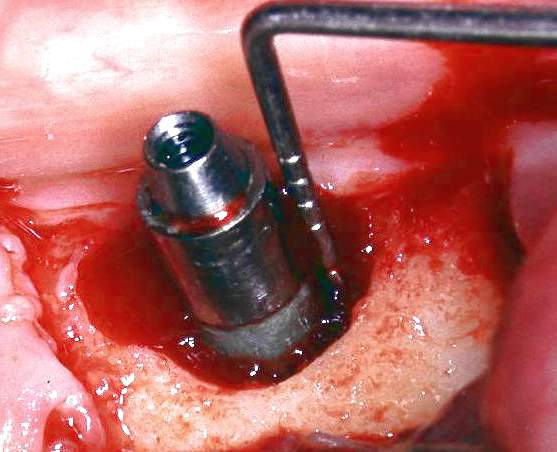
Dr. Balshi: We connect a transducer directly to the implant fixture.
Osseonews: In essence you are measuring the stiffness or rigidity of the implant to bone interface.
Dr. Balshi: That is correct.
Osseonews: So with these accurate measurements you can make decisions about primary stability with confidence.
Dr. Balshi: It especially enables us to make decisions about cases where the bone density is less than desirable and where we have to determine whether we should connect the implant fixture to the prosthesis or if we should just allow it more time to integrate more.
Osseonews: This kind of evaluation would be more important for cases with less dense bone.
Dr. Balshi: We would like to all have the perfect bone morphology and density for implant placement. When that is not the case – as it often is – we need to be in a position to derive the most accurate information we can get about the implant to bone interface. This is where the true value of RFA is apparent. This enables us to make the best possible decisions about treatment.
Osseonews: By comparison, tapping on the implant and evaluating the kind of thud it makes to determine primary stability really pales.
Dr. Balshi: Listening for a thud or testing the implant with a torque wrench provides some information. But the RFA approach is non-invasive and provides highly accurate information, which you can quantitatively measure the changes over time, and is an excellent research tool.
Osseonews: For those wanting more information on RFA, where should they look?
Dr. Balshi: The best reference is: A resonance frequency analysis assessment of maxillary and mandibular immediately loaded implants. Balshi SF, et al. International Journal of Maxillofacial Implants 2005;20:584-594. Glenn Wolfinger and I are coa-authors. This provides a description of the technique as well as the science behind it.
Osseonews: It is very clear that computerized technology plays an important role in your protocols.
Dr. Balshi: Yes and it is important for your readers to understand that we do not simply advocate or trying a technique without the proper training. It is essential to understand the techniques in their entirety so you can apply them. We give courses at the Institute in understanding and using the computer technology and software applications. If you do not truly understands how the whole system works, you might want to consider spending more time learning about it before using it.